By Nadia Paola Rodriguez Mendoza
Environmental Women ORG / Youth4Climate Project

In my community, climate change is not only measured in degrees, rainfall, or scientific projections. We feel it in the body. We see it in the fever of a child during the night, in the tired face of a woman who walked long distances to collect water, and in the fear of families who know that floods, droughts, and stagnant water can quickly become illness.
For the Narakajmanta Indigenous community in the Colombian mountains, climate change has become a health emergency. Women, girls, and LGBTI people who collect water are especially exposed to climate-related diseases such as dengue, chikungunya, malaria, Chagas disease, schistosomiasis, and leishmaniasis. When water becomes scarce, people must walk farther. When floods arrive, stagnant water expands. In both situations, disease vectors find new conditions to reproduce, and families with limited access to health services face the consequences.
This is why we started the ETHNOPROGRAM FOR CLIMATE MANAGEMENT OF HEALTH IN THE COLOMBIAN ANDEAN MOUNTAINS, supported by Youth4Climate and implemented by Environmental Women ORG together with the Narakajmanta Indigenous community. Our goal is to reduce the impact of climate-aggravated diseases among 5,000 Indigenous women, girls, and LGBTI people by creating a community-based, Indigenous-led model that connects climate adaptation, health care, prevention, and local governance.
At the center of this work is the creation of a Climate-Integrated Health Center: a space designed to improve early detection, basic care, prevention, and rapid response to diseases that are becoming more frequent and more dangerous because of climate change.

Why this project matters to me
I decided to lead this project because I have seen how climate change affects Indigenous women in ways that are often invisible in official reports. In many communities, women are the first to face the impacts of water scarcity, disease, and care responsibilities. They are the ones who walk for water, care for sick children, and try to protect their families when the health system is too far away.
For me, climate justice means that these women should not be treated only as victims of climate change. They must also be recognized as leaders, monitors, educators, and decision-makers. That belief shaped this project from the beginning.
We wanted to build more than a clinic. We wanted to build a community response system.
What we have achieved so far
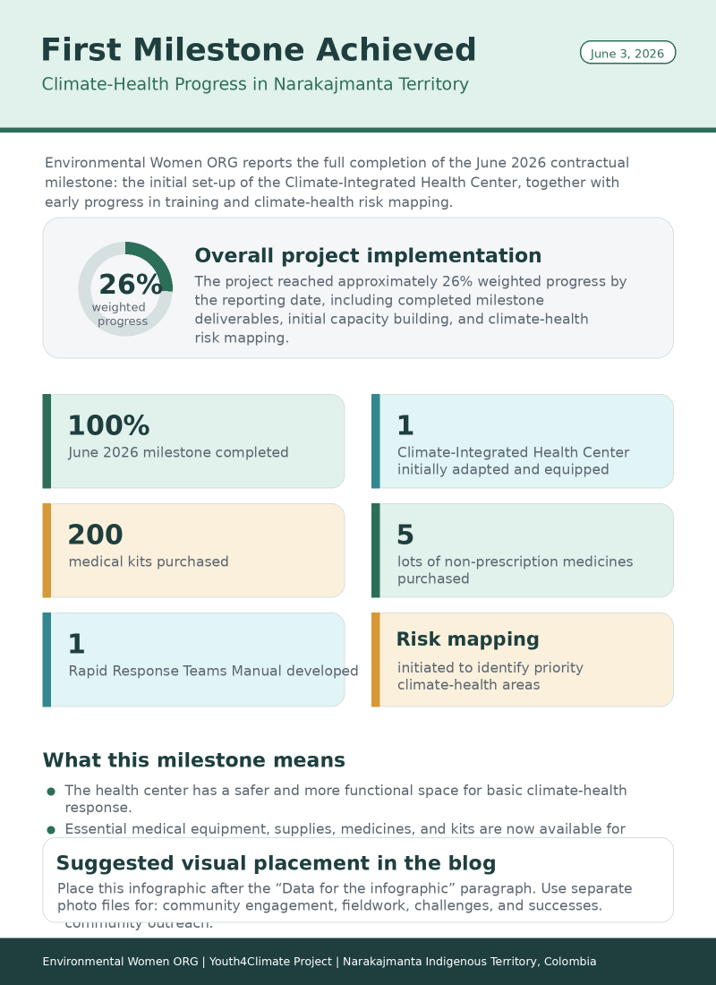
By June 3, 2026, the project had reached approximately 26% weighted implementation progress. This progress includes the successful completion of the first major milestone: the initial set-up of the Climate-Integrated Health Center.
During this first phase, we adapted the physical space of the center using counterpart resources. The site was improved with epoxy paint, better lighting, furniture, and health-appropriate construction materials. These improvements created safer conditions for basic health attention, medical organization, and community support.
We also purchased essential equipment and supplies, including stretchers, separators, a glucometer, thermometer, stethoscope, Doppler equipment, additional minor medical tools, five lots of non-prescription medicines, and 200 medical kits. These purchases allow the center to begin functioning as a practical space for prevention, basic diagnosis, and early response.
PHOTO 3 — Fieldwork: Team members: they medical kits, checking equipment, adapting the health center and preparing supplies.
For us, each medical kit represents more than a purchased item. It represents the possibility of responding faster when someone has symptoms. It represents a step toward reducing the distance between Indigenous families and basic health support. It represents dignity.
The project also advanced in two additional areas: initial community training and mapping of climate-health risk zones. Mapping is essential because the health risks are not the same everywhere. Some areas are more
The project also advanced in two additional areas: initial community training and mapping of climate-health risk zones. Mapping is essential because the health risks are not the same everywhere. Some areas are more affected by flooding, others by drought, and others by limited access to safe water. By identifying these zones, we can better prioritize future prevention, training, and response actions.

Rapid Response Teams: preparing before the emergency
One of the most important achievements of this phase was the development of the Rapid Response Teams Manual. This manual establishes the criteria, templates, schedules, and procedures for selecting and organizing community rapid response teams.
The purpose of these teams is to act quickly when there are outbreaks or warning signs of climate-related diseases. The selection criteria include community commitment, knowledge of the territory, availability to participate in training and emergency activities, communication skills, respect for health and ethical protocols, and validation by community leadership.
This is important because in remote Indigenous territories, waiting for external help can take too long. A local response system can save time, reduce risk, and strengthen community confidence.

Challenges we faced and how we responded
The first challenge was practical: transforming an available space into a safe and useful health environment. Instead of waiting for perfect conditions, we used counterpart resources and community effort to adapt the center step by step. This allowed us to move forward without delaying the project.
The second challenge was logistical. Medical equipment and supplies must be purchased, organized, documented, and stored carefully. We responded by keeping receipts, organizing evidence, and documenting the process through photos and videos.
The third challenge was territorial. Climate-health risks are dispersed across the community. Some families are more exposed because of their location, water access routes, or proximity to areas where disease vectors reproduce. The mapping process helped us understand these differences and prepare for more targeted action.

The lesson we learned is that climate-health work must be both technical and community-based. Medical supplies are necessary, but they are not enough. A health center must be connected to people, territory, knowledge, and trust.
Community voices
“Before this project, many families felt that climate-related diseases arrived faster than help. Now we see that the community is preparing itself, with a health center, medical kits, and young people ready to respond. For us, this is not only about health; it is about dignity and protection for our territory.”
— Estefany, NARAKAJMANTA Indigenous leader
“Participating in the mapping of risk areas helped us understand that climate change is also a health issue. Floods, droughts, stagnant water, and long walks to collect water are connected to the diseases affecting our families. Now we can identify the most vulnerable areas and organize prevention before the emergency becomes worse.”
— Bernie, NARAKAJMANTA Indigenous leader
“The Climate-Integrated Health Center gives us hope because it brings prevention and basic care closer to the community. Seeing the space prepared, the equipment purchased, and the response teams being organized makes us feel that Indigenous women are leading a real solution for our people.”
— Euladia, NARAKAJMANTA Indigenous leader
These voices are important because they remind us that impact is not only counted in numbers. It is also seen in confidence, participation, and the feeling that the community is no longer waiting passively for solutions.
Data for the infographic
The project has reached several measurable results during this first phase:
- 26% weighted implementation progress achieved by June 3, 2026.
- 100% completion of the June 2026 milestone.
- 1 Climate-Integrated Health Center initially adapted and equipped.
- 200 medical kits purchased.
- 5 lots of non-prescription medicines purchased.
- Essential medical equipment acquired, including diagnostic and basic clinical support tools.
- 1 Rapid Response Teams Manual developed, including criteria, templates, schedules, and operational guidance.
- Climate-health risk mapping initiated to identify priority areas for future response.
What comes next
This first phase gives us the foundation to move into the next stage of implementation. The next steps include strengthening the operational capacity of the health center, continuing training activities, consolidating community monitoring, and preparing the Rapid Response Teams for future activation.
We will also continue documenting the process through photos, videos, testimonies, and field evidence. This documentation is not only for reporting. It is also a way to show that Indigenous women and youth are leading practical climate solutions from their own territories.
For Environmental Women ORG, this project is a path toward a different way of understanding climate action. Climate action is not only about protecting forests, reducing emissions, or responding to disasters after they happen. It is also about protecting the health of communities before the emergency becomes irreversible.
In Narakajmanta territory, climate change has become a fever. But with community leadership, Indigenous knowledge, medical tools, and youth-led response, we are learning how to treat that fever before it becomes a crisis.

+ There are no comments
Add yours